Background
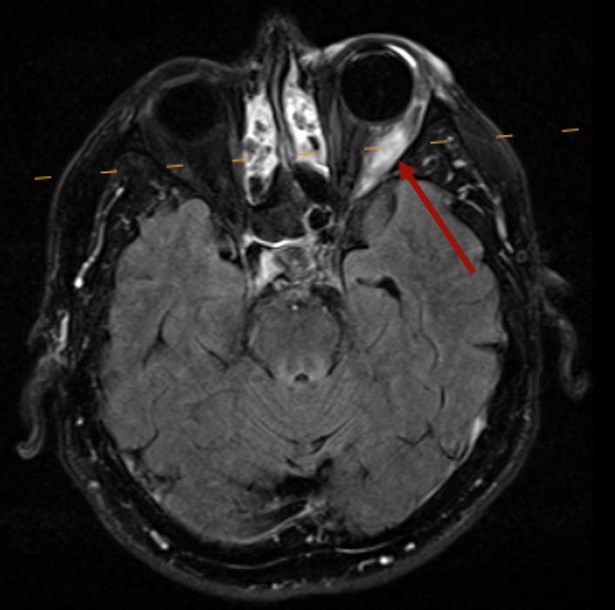
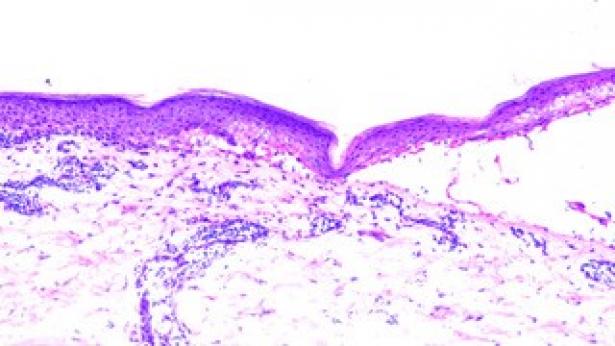
Myositis is a rare side effect of immunotherapy, occurring in <1% of patients and potentially fatal. An overlap with myocarditis and mysthenia gravis-like symptoms has been described. Diagnostic clues are provided by symptoms (muscle weakness, myalgia), increased CK, a myopathic pattern on electromyography, contrast uptake on MRI, and inflammatory or necrotic changes on muscle biopsy. Antibodies are mostly negative. Usually, immunotherapy should be interrupted or discontinued and systemic corticosteroid therapy (1-2 mg/kg) initiated. If therapy is refractory, plasmapheresis or IVIG, infliximab, MMF, MTX, or azathioprine can be initiated (Moreira et al., Eur J Cancer, 2019; Moslehi et al., Lancet, 2018; Kostine et al., Ann Rheum Dis, 2021).
Interestingly, in contrast to our case, three published cases of ocular myositis showed CK elevation (between 1844 and 7765 U/L), possibly due to involvement of other muscles. The 3 cases were treated with corticosteroids; in 1/3 of the cases the anti-PM-Scl 75 antibodies and anti-SRP antibodies were positive and plasmapheresis was also performed. In all three cases, the symptoms improved or resolved (Garibaldi et al., Neuromuscular Disorders, 2020; Kamo et al., BMC Neurology, 2019).
In the differential diagnosis, ocular irAE (e.g. conjunctivitis, secleritis or unveitis) also had to be considered initially. Ocular irAE occur in approximately 1% of patients receiving ICI therapy and non-muscular ocular irAE can often be treated topically, so interruption of ICI therapy may not be required.