- 1978 uveal melanoma right eye, HLA-A*02 negative, IV (AJCC 2017)
- 04/2021 cutaneous melanoma, IA (AJCC 2017)
- 09/2021: subcutaneous melanoma metastasis
- 11/2021: liver melanoma metastasis, BRAF wild type
- Both metastases probably associated with uveal melanoma (histologically)
- 01/2022 – 02/2022 Combined immunotherapy with ipilimumab 3 mg/kg + nivolumab 1 mg/kg (3 doses)
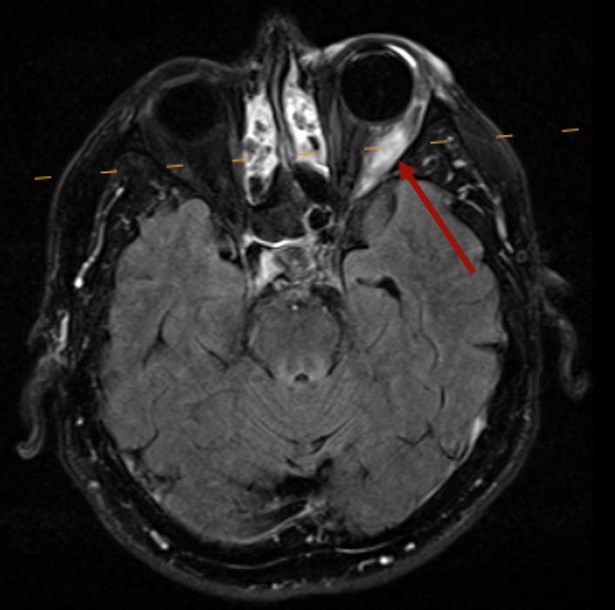
After 3 doses of combined immunotherapy with the immune checkpoint inhibitors (ICI) ipilimumab and nivolumab, the patient presented with a burning sensation and swelling in the left eye. The ophthalmological emergency service suspected conjunctivitis, so corticoid-containing eye drops and eye ointment were used, but the swelling continued to increase. An ophthalmological examination revealed impaired ocular motility, so a cerebral MRI was performed, which revealed inflammatory changes (swelling, edema and contrast uptake) in the left lateral rectus muscle and an exophthalmos. An ipilimumab/nivolumab-induced myositis of the lateral rectus muscle was diagnosed. The creatine kinase (CK) was in the normal range.
We initiated a systemic therapy with prednisolone with an initial dose of 2 mg/kg, which was soon reduced to 1 mg/kg and then tapered off. Just two days after the start of the prednisolone treatment, the swelling had completely subsided; ocular motility also returned to normal over time. After tapering off the prednisolone to 10 mg, irColitis developed, which had to be treated with infliximab due to a steroid-refractory course.
Up to now, staging has shown stable disease, therefore immunotherapy was not reinduced due to the potential exacerbation of the steroid-refractory colitis. If necessary, reinduction should be carefully evaluated.
Myositis is a rare side effect of immunotherapy, occurring in <1% of patients and potentially fatal. An overlap with myocarditis and mysthenia gravis-like symptoms has been described. Diagnostic clues are provided by symptoms (muscle weakness, myalgia), increased CK, a myopathic pattern on electromyography, contrast uptake on MRI, and inflammatory or necrotic changes on muscle biopsy. Antibodies are mostly negative. Usually, immunotherapy should be interrupted or discontinued and systemic corticosteroid therapy (1-2 mg/kg) initiated. If therapy is refractory, plasmapheresis or IVIG, infliximab, MMF, MTX, or azathioprine can be initiated (Moreira et al., Eur J Cancer, 2019; Moslehi et al., Lancet, 2018; Kostine et al., Ann Rheum Dis, 2021).
Interestingly, in contrast to our case, three published cases of ocular myositis showed CK elevation (between 1844 and 7765 U/L), possibly due to involvement of other muscles. The 3 cases were treated with corticosteroids; in 1/3 of the cases the anti-PM-Scl 75 antibodies and anti-SRP antibodies were positive and plasmapheresis was also performed. In all three cases, the symptoms improved or resolved (Garibaldi et al., Neuromuscular Disorders, 2020; Kamo et al., BMC Neurology, 2019).
In the differential diagnosis, ocular irAE (e.g. conjunctivitis, secleritis or unveitis) also had to be considered initially. Ocular irAE occur in approximately 1% of patients receiving ICI therapy and non-muscular ocular irAE can often be treated topically, so interruption of ICI therapy may not be required.
Ocular myositis is a rare side effect of immune checkpoint inhibitors that physicians should be aware of and that requires ICI therapy interruption and systemic corticosteroids.