- 01/2021 non-small-cell lung cancer (adenocarcinoma)
- Initial stage: cT2N0cM0, IIB, PD-L1 expression 10%
- 01/2021 – 03/2021 Radiochemotherapy with cisplatin, vinorelbine and radiation 66,6 Gy
- Partial response
- 05/2021 - 02/2022 Immunotherapy with durvalumab 10 mg/kg bw every 2 weeks (19 doses)
- Partial response
After 9 months (and 19 doses) of immunotherapy with the anti-PD1 antibody durvalumab 10 mg/kg bw every 2 weeks, the patient developed a “rash”. Initially, the immunotherapy was discontinued and the patient treated with topical steroids and systemic prednisolone 60 mg p.o. for 10 days, which led to an initial improvement of the skin condition. While tapering the steroids, there was another exacerbation and 150 mg prednisolone i.v. were administered. Since there was no improvement under this therapy, the patient was referred to the department of Dermatology.
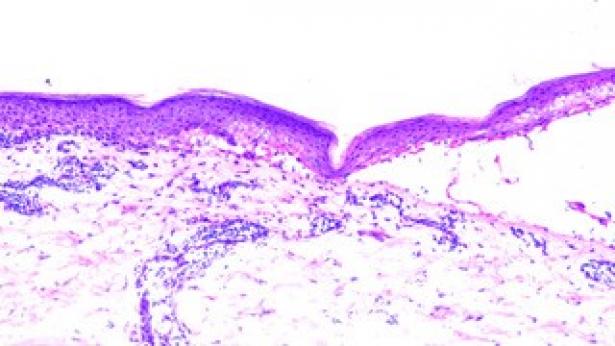
The patient presented with erythema and erythematous plaques covering approximately 18% of the body surface area, predominantly on the distal extremities. There was also lamellar desquamation and blistering, particularly on the hands. Histology showed vesicular detachment at the level of the basement membrane zone, a perivascular lymphocytic infiltrate, single-cell apoptosis and single eosinophils. The fluorescence pattern was non-specific. In summary, the findings corresponded to an erythema multiforme (EM)-like drug reaction.
The dose of corticosteroids was increased to 250 mg prednisolone i.v. for 3 days and then reduced to 80 mg p.o. The steroids were then tapered very slowly, but had to be increased again twice. In parallel, topical therapy with mometason cream was carried out. Due to the steroid-refractory or steroid-dependent course, secondline immunosuppression (therapy with intravenous immunoglobulins (IVIG) as well as extracorporal photophereses) was discussed.
Four months after the onset of the erythema multiforme, currently, a cortisone dose of 30 mg is required. Secondline immunosuppression was not started and the checkpoint inhibitor therapy was not yet re-initiated.
Cutaneous side effects are observed in 46-62% of patients on checkpoint inhibitor therapy and occur after a median of 2-3 weeks, but also up to two years after the start of immunotherapy. Rash, pruritus, and vitiligo-like lesions are the most common; lichenoid reactions, blistering reactions, psoriasis, and sarcoid-like lesions are less common. In 90% of cases, cutaneous irAE are mild and can be treated with topical therapy. Serious and potentially fatal cutaneous adverse events include DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms), Stevens-Johnsons Syndrome, toxic epidermal necrolysis, bullous skin lesions, and dermatitis herpetiformis (Heinzerling et. al, Dtsch Arztebl, 2019; Belum et. al., Eur J Cancer, 2016). The literature on erythema multiforme under immunotherapy is limited to individual case reports. Cases have been reported with ipilimumab, nivolumab and pembrolizumab. Treatment was mostly with systemic steroids, in one case also with IVIG. EM often led to discontinuation of immunotherapy (Zimmer, L et al, J Transl. Med, 2015; Jour et. al., J Cutan Pathol., 2016; Sundaresan et. al., Dermatol Online J., 2017; Utsunomiya et. al., Case Rep Dermatol., 2018; Yano et. al., Trends in Immunotherapy, 2021; Hashimoto et al, J Clin Med., 2021; Ambur et. al., Cureus, 2021).
Cutaneous irAEs are often mild but can be severe, requiring discontinuation of immunotherapy and initiation of systemic therapy. Dermatologists should be involved in managing cutaneous side effects, since specific skin findings may require varying treatments.